|
|
Call 07361805089
|
Blog
|
|
Call 07361805089
|
 Diagnosis is a funny old thing. It can tell you everything...and nothing. It comes from Greek roots meaning to 'know or recognise' and 'apart'. We tend to think of our bodies like a machine, on which we can run a diagnostic check and find the cause of our pain and or disability. A blood test for this and a scan for that. This is what is wrong and this is what we do to fix it...or not. Osteopathy has 4 central tenets and one of them is particularly relevant here...'the body is a unit'. what does that mean and why is it so important? It means that we are looking at the interaction of structures and systems, the function of the whole not the part. The reason we sometimes get seemingly miraculous results, where others have failed is because we cast our net wider, looking for (often multiple) predisposing and maintaining factors. If someone has tennis elbow (that is inflammation of the point where the tendons of the forearm muscles attach to the outside of the elbow) we can treat it with anti-inflammatories, even steroids and the pain will go away, great! But why did it occur now and in that arm? Unless there is an underlying condition and often, even then, it is because the muscles are pulling on the area too much, meaning they are too tight or are being overused and so, if we don't reduce the tension on the muscles or adjust our activity to reduce the overuse then the pain will return as soon as the anti-inflammatories wear off. OK so we massage the forearm and give some stretches and say to lay off the tennis. Why now though? I've been playing tennis for years...and I've stopped for 3 weeks and the pain went away but as soon as I started again it came back...Will I have to give up for good? Muscles rarely become too tight for no reason, something else has changed that has resulted in that, so we look at the wrist and see if it is functioning properly, because the muscles of the forearm nearly all cross the wrist and dysfunction there can lead to tennis elbow, and then we look at the shoulder. Is the shoulder, rounded, which means the forearm needs to supinate (turn out) to present the hand neutrally? If the shoulder is rounded, why? Is it because the ribcage isn't operating properly and the shoulderblade is tipped forward over prominent ribs below, is the ribcage dysfunction due to a scoliosis, is that structural (skeletal and not easily changed) or functional (functional and caused by either a soft tissue tightening in the torso or an apparent leg length discrepancy). If there is an apparent leg length discrepancy, what is causing that, is that because of a pelvic torsion, either soft tissue or an actual sacroililac joint shift or is the arch of one foot becoming flattened and is that permanent or the result of an ankle dysfunction?
So actually, the diagnosis of tennis elbow, is not that useful. The real problem is the sprained ankle that wasn't properly resolved and the knock on from that. Altogether now..."The hip bone's connected to the thigh bone"
0 Comments
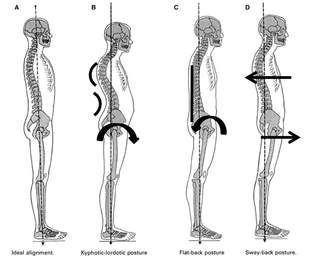 A month ago The BBC ran an article on complaints about how hard the new Thameslink train seats are (see it here, it also features the first osteopath I’ve ever seen asked to give his expert opinion). I’ve had the opportunity to ride one of them now and can confirm that, in a modern world of uncomfortable public seating, these are the worst so far. They are very hard, very upright and quite straight in the back. “Surely sitting straight and upright is good for you?” I hear you cry…I’ll come back to whether it is good for most of the population later but it most certainly is not good for anyone who cannot comfortably hold that position.
The problem is that not everyone has an “ideal” shaped back. Many people, including myself have increased curves…they are kypho-lordotic. They are not necessarily just slouching. They may have developed wedge-shaped vertebrae, either as a teenager (common amongst those with a fast growth spurt) or in older age due to osteoporosis; others just may no longer be able to straighten, as soft-tissues in the chest (muscles, tendons, fascia, ligaments) have shortened over time as a result of hours at a desk, or even over-work of the chest relative to the back, at the gym. An upright seat, hard padding with no give and a back that cannot straighten means that the passenger will be sitting with their head tipped forward, that is 4-5kg pulling forward and needing constant support from the muscles of the neck and back. Evidently that is a potential recipe for pain and dysfunction. On 5 March the Guardian ran an article stating that there was little evidence connecting back pain with slouching and bad posture (read it here). It was a confusing mess of clearly contradictory definitions of posture – quoting an osteopath (another one), a ballet teacher and a physiotherapist. Worryingly the article suggests that workstation assessment was about sitting up straight and that sitting up straight was not particularly useful. My suspicion is that the journalist has got a number of different quotes and weaved them together but has confused three different things
 I have been taught like a good British School of Osteopathy graduate to come up with a diagnosis.
I listen to your explanation of where the injury is located, what happened when the injury occured, what has happened since, the nature of the symptoms etc and then I examine you, looking for physical signs of injury or inflammation, or infection, or just musculoskeletal assymetry or altered movement patterns. All of this is to determine the tissue causing the symptoms. Except there is rarely one tissue causing the symptoms. So I use the time-honoured format of including pre-disposing factors and maintaining factors in my diagnosis. The pre-disposing factors are those which are musculoskeletal and maintaining are others, such as lifestyle factors, poor mattress, stressful job etc. Sometimes the list is extensive and it is like the song 'there was an old woman who swallowed a fly' with the problem getting bigger and bigger as insult piles upon injury, except that to make it more complicated you're often not quite sure in which order the injuries happened. I only have to look to my own body for an example I have a flexed area between t5 and t8, I've had problems with my shoulders, painful ribs and also pain lower in my back at the TL and in the left sacroiliac joint...oh and tight hip flexors. How do I, or my osteopath, deal with all of that? We could either treat them as unconnected or try and find a plausible story to link them together. Why would that be useful? It is useful to understand which problems are connected because one may have been caused by another and in turn may prevent the other from resolving fully unless it receives attention also, likewise if the initial insult isn't dealt with the newer problem may recur, even if it has been fully resolved, the pre-disposing factor hasn't been removed. It makes sense to me to prioritise the newest injury first, that way you are returning to a state you know the body was able to inhabit for a while, even it it may not be sustainable in the long-run. Removing the initial insult, if possible, would be to take the body to a new condition and may result in further compensations and new injuries. So how does this apply to my body? I think there are 2 groups. I think the Sacroiliac Joint, hip flexors and TL are the newest group, dating back to an SIJ injury in Jan 2017. They are almost self-contained...except the TL dysfunction causes both twelfth ribs to, for want of a better word, get stuck and increase the tension in my rib cage related to the rib problems higher up The T8 area relates to an injury about 5 years ago and actually appears to be one joint rotated left and another rotated right and both pulling in opposite directions the T5 area injury is a joint that is stuck flexed (unknown timespan, at least 8 years) with associated ribs either side which sit are pushed proud of the bulk of the rib cage and cause tight intercostal muscles, and tipping forward of the shoulder blades, this in turn causes muscle pain from muscles which are permanently on stretch, I feel this most in the back part of the armpit where it joins the torso. The tipping forward of the shoulder blade also causes mechanical disadvantage to the shoulder and increases the chance of subacromial impingement and inflammation and also of muscle injury, particularly to the rotator cuff muscles and lo and behold I have had exactly those problems. So where to start? Start with the newest problems, so the Sacroiliiac joint, hip flexors and TL, as a discrete set of problems they are quite manageable as a group for treatment and I am pleased to say have nearly fully resolved. The Problems around T8 next, they are very near to resolving also. Meanwhile work on the ribcage has been much more productive since the TL issue and the associated twelfth rib mediated tightness has gone, the 5th ribs are sitting a little flatter and the shoulderblades are less tipped. All this means the shoulders are starting to recover...but I'm well aware that this can't stop until the T5 issue is resolved, otherwise I will always be prone to bad shoulders and it may even be that the lack of movement through T5 area was a predisposing factor for the T8 TL or even the left SIJ injury. So don't be surprised if you come to me with a bad shoulder and I'm interested in your pelvis. I may need to find the spider to remove the fly!  I allow an extra 30 minutes for your first visit...Why? To ask you questions.
I'll be asking you all about the issue that has brought you to me and also about your health in general. Why is that? 1. To make sure your issue is appropriate for osteopathic treatment today Osteopathy started out as a form of medicine for all systems of the body...but I am trained to use osteopathy to help patients with mechanical musculoskeletal problems, and whilst I am very happy to support patients who have other conditions, I don't purport to treat those conditions, so it is my responsibility to refer patients outside my remit. Many systemic conditions present with musculoskeletal symptoms and the case history I take is designed to detect these, so if you are complaining of low back ache and I seem interested in whether you have problems urinating I am thinking about the possibility of a kidney problem or prostate cancer that has metastasised to the lumbar spine. If you are a woman and I am asking about your periods then I might be wondering if you have fibroids. There are few absolute barriers to treatment but an example might be someone with calf pain and the history tells you it started after they returned from holiday...a quick look and very gentle touch to confirm that there is a pulsatile mass and straight off to A&E to investigate for Deep Vein Thrombosis. 2. To determine what forms of treatment are appropriate If you have had a lifetime of steroid use, or long term anorexia, or a series of broken bones for relatively small knocks, I need to know because it suggests you may have lower than normal bone density. If you have low bone density, I will use more gentle treatment, even if it means results take a bit longer. If you have problems which suggest you might have some cardiovascular disease then I will be even more careful when treating your upper neck, I don't want to run the (tiny) risk of breaking off an atherosclerotic plaque. 3. To identify what the problem is. By asking you questions about how the problem occurred, how it then progressed, what aggravates it or relieves it, where it hurts and the nature of the pain, I am usually able to work out what is likely to be wrong before I even start to examine you. The examination is designed to add weight to the diagnosis. I don't have X-ray or MRI eyes, or access to nerve block injections so my diagnosis is provisional and the strongest piece of evidence for what is wrong with you is usually the case history. I'll give you an example. A man, in otherwise good health, walks in with low back ache. The pain is worse for movement, especially extension and rotation, standing is painful but sitting not so much, no pain into the legs. The injury occurred in the gym 2 days ago when he bent over a little and felt it go, he was in instant pain and couldn't straighten up, the pain has got a bit better since. The injury had a clear onset and was as a result of movement. It is also aggravated by particular movements and the man is otherwise in good health, this tells me that the problem is almost certainly musculoskeletal and mechanical in origin. I think it very unlikely it is a herniated disc since the injury happened at partial flexion, not full, the pain was instant rather than taking several hours to develop, no pain into the legs (disc bulges often press on the peripheral nerves, which, in this area, innervate the legs), pain in all ranges of motion, not just flexion, pain not worse for sitting (or all weight-bearing activities) and starting to recover within a couple of days. All of these point me away from a disc injury. I also doubt it is a muscular or ligamentous tear as it didn't occur when under heavy load, so I am thinking that it is likely to be a facet joint injury, some further testing and I am able to confidently estimate recovery time and i can use this knowledge to inform the treatment I use 4. To get to know you I could send you a health questionnaire and save time and room hire fees. I don't because sometimes I get additional information about a person, that they wouldn't put on a form. Our health, or otherwise, is determined, not just by our physical presence or absence of dysfunction but also our psychological state, our social relationships and our lifestyles. This isn't airy-fairy. If you are stressed you pump out cortisol. Cortisol is designed to keep you keep you ready to fight or flight, this process reduced the resources available to repair injuries. If you have just changed job and the seat is uncomfortable. If you have a 2 year old who is heavy but demands to be carried. Whether you smoke, drink too much, eat poorly, or are a paragon of virtue. All of this information is important to me and is difficult to get from a questionnaire. Just as importantly though, it is a chance to get to know me a little too...it is an ice-breaker. It is uncomfortable enough, for many, to undress to their underwear for examination. At least this way we are not quite strangers by that stage,  Christmas is over and the turkey wasn't the only thing that got stuffed. Many of us over-indulged in both food and alcohol and have come out the other side swearing to shape up...but we should be realistic about the shape we are currently in, and chose our exercise regimes accordingly! I am specifically thinking about the suitability of running as exercise for the unfit, overweight, or under-prepared.
Don't get me wrong, running is clearly fantastic exercise, it takes the weight off, gets the heart pumping, helps maintain bone density and improves general fitness but it is also high impact. That means it has the potential to impact heavily on a number of structures and do us more harm than good, so here are a few things to think about
So how does this depressing litany help us train smarter and more safely?
I'm going to get it out there. I can't help your slipped disc! A slipped, or herniated, disc is a protrusion of the soft inner matter of the intervertebral disc, through the outer fibrous layer and no amount of osteopathy (or anything else) is going to poke it back in. That doesn't mean I can't reduce your pain or increase your function as you deal with a slipped disc.
Slipped discs 101 As I mentioned above, the slipped disc occurs when the outer fibrous part of the intervertebral disc, the annulus fibrosis, breaks down and the fibres fray and part, allowing the inner liquid, nucleous pulposus, to create a bulge in the wall of the disc and sometimes to extrude. As the bulge occurs and some of the matter from the centre of the disc is displaced outwards the disc loses height and the ligaments muscles etc acting over the joint are all now too long to provide full stability, the body can respond to this perceived instability by tightening up all of the muscular tissue around the joint to protect it and make it immobile, this can be painful and can impair function. The loss of disc height and tightening of muscles can also bring into contact other structures which are meant to sit in close proximity but not touch, and they can become irritated and inflamed, as a result. The most common pain that suggests a possible slipped disc is pain down the leg...so called sciatica...I say, 'so called' because a true slipped disc will cause irritation to a nerve root instead of to the peripheral nerve (sciatic or otherwise) and the pattern will be slightly different but that's nerd stuff. I have had patients tell me that their problem is due to a slipped disc...it must be...I had an MRI and the report says I have a slipped disc at L1-L2, the trouble is, their symptoms are consistent with S1 nerve root irritation...nerd stuff again...basically the slipped disc is far too high to give them the symptoms they are experiencing. 27% of over 40s without symptoms have herniated discs, maybe in multiple, so this tells us that many herniated discs don't cause pain. Back pain, even back pain that mimics a 'slipped disc', can be caused by many different dysfunctions, either singly or in multiple. What does this tell us? That there is a lot of uncertainty in diagnosis and even more in prognosis. So why bother to try and work out whether an injury is discal in origin? The first is an issue of safety. Disc prolapses are usually painful rather than dangerous but sometimes they compress the nerves in the spinal canal (another nerdy fact, the spinal; cord ends before the low back and here the nerves in the spinal canal are called the cauda equina as they run separately like the hairs in a horses tail). If there is a likely disc prolapse it is useful to make the patient aware of the symptoms to look out for if rare but dangerous cauda equina syndrome is occurring. Secondly, I would modify my techniques where I suspected a disc prolapse. The chances of an osteopathic technique exacerbating a disc issue are slim but let's reduce that chance even further by selecting techniques that minimise the risk. Finally, the patient needs to know the possible prognoses (plural), a disc herniation can take a long while to heal and may not respond to osteopathic treatment, the chance of a complete cessation of symptoms in the short term is lower than for some other types of back ache, that doesn't mean it can't happen but it is important that the patient has realistic expectations of treatment. Overall I have been pleasantly surprised how well many patients who have had classic slipped-disc symptoms and signs have responded to treatment despite the fact I can't 'pop the disc back in' The curious incident of the pain in the bum in the night time - a diagnostic detective story24/10/2017  I thought you might like an example of the thought processes I go through to determine what needs treatment to resolve somebody's pain or dysfunction. This is the story of someone in their mid forties with no known underlying health issues who woke up one morning after a night in bed asleep and alone, with severe pain in their bottom region. The pain was and is enough to make them yelp during certain movements, it really hurts!..I know this because this patient is me and the morning was yesterday.
Yesterday I woke and immediately felt it, lying in bed; a sharp pain in my...was it my coccyx? When I got out of bed I yelped because it hurt so much. OK, so the coccyx doesn't usually become painful for no apparent reason. Had there been a fall, or other trauma to the area? No trauma, in fact I'd had a lazy day the day before (Sunday) and spent most of it on the sofa. I had been decorating and been out dancing the day before but had no pain following that. No trauma, doesn't sound like coccyx. Do you have a history of problems with the coccyx? No Or pelvis? I hurt my left sacroiliac joint 9 months ago, actually it ached a bit in bed and I had a bit of sciatica a couple of nights last week. Do you have any sciatica now? No! It was just a couple of nights last week. OK. So what movements and positions hurt now? Lying in bed, sitting and walking hurt, but standing is OK. Actually sitting is OKish, it is standing from sitting that really hurts, that's when I yelp. Coughing sneezing and going to the toilet are pretty yelp inducing too. But there are no issues with being able to go to the toilet? Only braving the discomfort Does anything make it better? Ibuprofen You said lying in bed was bad, can you get comfortable to sleep? If I lie on my right side with my left leg forward I am comfortable but I tend to move in the night and then the pain wakes me. I had to get up at 4am for an ibuprofen last night So the pain wakes you at night? You've not had any night-sweats, unexplained weight loss, nausea or change in appetite, constant fatigue, blood in urine or difficulty peeing, have you? No OK, lets have a look at you. Now bear in mind I can't see myself from the back but I can't feel any puffiness and my low back doesn't feel affected so my suspicion is there is little visible asymmetry. None of the joints of the lumbar spine are tender to palpate and neither are either of the sacroiliac joints. The sacrococcygeal joint, however is very tender on both the left and right side. The coccyx itself isn't. Lets try some movements Well obviously rising from sitting hurts. Surprisingly though rotation right is the most painful spinal movement, actually bending forward and straightening from that doesn't hurt much. Right hip no pain on any movements but left hurts at full extension (moving leg back) and a bit on internal rotation of hip. I can only test these actively on my own, so using muscles, but on a patient I would then test the painful movements taking the joint through the range of motion with the body relaxed, so if it still hurt I would know it isn't muscles. In this case I know it isn't muscles because it hurts sitting and lying still. For a little while I was a bit stumped as to how the sacrococcygeal joint became so painful during the night, without trauma but i think the evidence above is enough for a pretty good hypothesis. We can be pretty sure it is the sacrococcygeal joint that is generating the pain. pressing on it hurts and releasing pressure on it, when standing from sitting, also really hurts (it isn't about the movement in this instance as standing from bending over is the same movement but doesn't hurt). Pain that awakens someone in the night and comes on for no apparent reason are a couple of red flags and can, in the presence of other symptoms or signs suggest that further investigation is required to ensure that, for example, there isn't metastatic bone cancer. In this case there are no night sweats, weight loss, fatigue, nausea or appetite change, all possible indicators of cancer and no difficulty peeing or blood in urine, perhaps specifically indicative of prostate cancer, the most likely cancer in men to spread to the lower spine. The pain is also movement related and that is a very strong indicator that it is musculoskeletal and mechanical. It is also responsive to ibuprofen, suggesting the process is, at least in part inflammatory. The saccrococcygeal joint is subject to anatomical variation. It can contain a disc, which can herniate, bulge or 'slip' but more likely may just be a simple synovial joint, or even may be ossified. Again red flags appear with difficulty going to the toilet, are nerves being compromised by a bulging disc?..Not in this case, it is just painful but there are no difficulties openoing or closing the valves, so to speak. The most common cause of pain at this joint is irritation of the soft tissues around the joint, ligaments, capsule etc...and what irritates those? Being stretched. How does that happen? Either the coccyx is held uncomfortably, or the sacrum is. We know that there has been no trauma to the coccyx and that it usually takes one for it to move, so that leaves the sacrum. The sacrum is a vaguely triangular bone which has joints with the coccyx at the bottom, L5 (the bottom lumbar vertebra) at the top and the ilium part of the innominate bones (main pelvic bones) at the sides. None of the other joints are painful but the history tells us that there has been a problem in the past with the left sacroiliac joint and that there may have been some recent disorder there, so it would make sense to think about whether that was likely implicated. Pain is worst (apart from when pressure is released) when the left leg is back (hip extended) and relieved when lying in bed with the left leg forward, it also hurts when lying on my back, where the weight of my leg is forcing the leg straight. If you've read the sacroiliac joint series in this blog you'll know that the evidence suggests the joint doesn't move much unless certain conditions are met, however my mechanism of injury 9 months ago opened the joint and rotated the left innominate posteriorly relative to the sacrum, which would have the potential to be in the category of those rare occassions when the joint actually does move out of alignment. It doesn't have to have moved much, but either not having fully resolved it at the time, or (perhaps having weakened ligaments when I hurt it last time) repeating the injury enough to move it a little but not to cause pain in the joint itself could lead to my sacrum being twisted between the innominates...and most importantly relative to the coccyx. bringing my leg back and even lying all night with it flat against the bed would increase that twist. So this is my best guess but all diagnosis is exactly that...a best guess. Phrases such as, 'we'll do a scan to make sure' give a false sense of certainty. A person may have a disc bulge at the right level but it may be asymptomatic and the pain may be driven by another structure. Certainly the orthopaedic tests we do have limited specificity and sensitivity and on their own can only form a small part of the picture, but when combined with the palpatory findings, anatomical knowledge and experience informing our perception of the likelihood of each scenario and most importantly the patient's history of this and previous ailments we can build a good picture and a reasonable diagnosis.  The traditional method of evaluating whether a treatment is beneficial in reducing pain is to measure it against placebo (a sham treatment that has no anticipated external beneficial effect) in a blinded trial (single, in this case, as it is a bit difficult to blind the practitioner as to whether they are giving real or sham treatment) and to use scales and questionnaires for patients to record their pain levels before and after treatment. Although the pain levels will be subjective the scales and questionnaires used are consistent and as such the results from a large population can be considered robust.
In this meta-analysis editorial complementary medicine sceptics Colquhoun (pharmacologist) and Novella talk about the lack of evidence of any consistent placebo exceeding effects in over 3,000 papers regarding acupuncture. Recent research by Richard Harris (co-president of the society for acupuncture research) shows that there is an effect on the neurotransmitters in the brain which is very different for real as opposed to sham acupuncture. With traditional placebo effects such as sham acupuncture additional endorphines are released which reduces pain, with real acupuncture the effect seems to be that more receptors are created instead and in disorders like fibromyaglia where there appear to be an insufficiency of receptors this suggests the acupuncture is not just providing relief but is actively curing the condition. Perhaps the problem here is that we think of placebo as non-intervention, when in fact it can be a very powerful intervention. This research suggests that the placebo effect does necessarily not operate in addition to other pain relief effects for all interventions and so other effects with different long term consequences to the placebo effect may be being masked by this comparison to the placebo. Also notice the highlighted fields of expertise. I am not implying improper conflicts of interest , lack of fairness or intellectual rigour, just a mind-set. If you are a pharmacologist comparing two pills, which look smell taste and feel the same but have different active chemical ingredients then 'placebo' is just background noise and the difference must be entirely due to the ingredients...one assumes! Likewise if your field of expertise is under attack as being nothing more than placebo then maybe you have a vested interest in understanding more about what placebo is. I've always been interested in the idea of degrees of placebo and in the different capacity to to initiate placebo in different people at different times using different means. If osteopathy were placebo, would it matter if it were better placebo (for some people) than ibuprofen and if the pain relief generated allowed normal behaviours which in turn allowed the body to better heal itself? Hang on! Isn't that the meaning of one of the central tenets of osteopathy 'the body contains its own medicine chest'. I'm not suggesting that osteopathy is 'just' placebo but now that we know the placebo effect is real and isn't always present in the same way and at the same magnitude (therefore can be reduced, turned off or increased), isn't it something we should be trying to understand better and shouldn't we be a little more critical in appraisal of effect versus placebo in future? this blog entry was inspired by an article in the Guardian here  A recent study by Public Health England suggested that 41% of Britons aged 40-60 fail to exercise so much as 10 consecutive minutes brisk walk each month. This is shocking, so much so that I have difficulty believing it, but even assuming it is an exaggeration it does highlight an underlying truth that a significant proportion of middle-aged Britons fail to do any significant exercise.
The focus in the media is on the benefits to your heart. By walking just 10 continuous minutes at a brisk pace every day, an individual can reduce their risk of early death by 15%. They can also prevent or delay the onset of disability and further reduce their risk of serious health conditions, such as type 2 diabetes, heart disease, dementia and some cancers. The human body is not designed to be sedentary, it relies on movement for far too much. Obviously it survive without movement, people do, but it can't function properly. There are so many systems which rely on movement some more obvious than others, here's a few, by no means the full list Joint health - The joints are lubricated by synovial fluid, this nourishes the cartilage which lines the joints, the synovial fluid is spread across the joint surface by a combination of one surface of the joint wiping the fluid across another and by the loading and unloading of joint surfaces causing alternate high and low pressure and pumping the fluid around the joint, both of these processes need movement (weight bearing for the latter). Bone health - Bone density responds to loading both direct loading from weight-bearing and from the pull exerted by muscles. Activity, preferably weight-bearing, is therefore important to maintain bone-density, Circulatory health - The heart is not the only circulatory pump in the body, in fact it is not really up to the job on it's own, it relies on other smaller pumps most of which are muscular and rely on activation of muscles through movement to aid venous return. If circulatory pumping is inadequate then there is the potential for stasis, this is how sitting still on a long flight can contribute to the development of a deep vein thrombosis as blood can start to clot when it isn't flowing. Stasis can also contribute to ulcer formation and even in extreme cases the thickening and weakening of the heart's muscular walls. Antibody response - Studies have demonstrated that the immune system also uses muscular pumping systems to speed up your antibody response to infection. Infective particles are presented and recognised quicker and antibodies are created and distributed more rapidly decreasing the time it takes to counter threats and giving them less time to multiply and increase their potential to threaten you. Enough time sat here writing this...I'm off for a swim, maybe you should do the same! I plan to add some recommended exercises to this site in the near future but until I do here is a really good and and well explained exercise to do before you train, or just during the day. The point is that it improves balance and proprioception in three dimensions. Three dimensional proprioception is critical since although our knees and ankles move most significantly in the anterior posterior plane we need strength, and more importantly quick automatic pretensioning reactions, in other planes in order to prevent knee and ankle sprains and strains. For those whose knees tend to drop inward when running, cycling or working out, this is also great since this will help you body build up appropriate strength, get used to firing the right muscles at the right time and understand where your limbs are in space in order to start to correct or limit that issue. This exercise will work a surprising range of muscles quite hard. We've talked about muscles around the knees and ankles but think about what is going on at the pelvis also.
No more spoilers, read Steve's blog and watch the video. It's not as easy as it looks, so take Steve's advice and perhaps try it holding onto a chair first. Click here |
Archives
February 2024
AuthorDamian is the principal osteopath at Vauxhall Village Osteopathy and Oval Osteopathy Categories
All

|

|

|

|
 RSS Feed
RSS Feed