|
|
Call 07361805089
|
Blog
|
|
Call 07361805089
|
 for low back pain. Actually they do but not very much. Hot on the heels of the Cochrane review demonstrating the lack of efficacy of paracetamol for low back pain the BMJ journal 'Annals of the Rheumatic Diseases' has published a systematic review with meta-analysis (a review of all of the papers out there and a combination and synthesis of the results) of Non-Steroidal Anti-Inflammatories for spinal pain and has found that although there is some limited demonstrated effectiveness it is not enough to be considered clinically important. They also found that use of NSAIDs increased the likelihood of gastrointestinal reactions 2.5 times.
I take ibuprofen when I need it, it is a very useful anti-inflammatory and painkiller so am in no way suggesting that these drugs are useless, but it is interesting to read these results and indeed the findings of the authors that 'At present, there are no simple analgesics that provide clinically important effects for spinal pain over placebo'. Read the abstract here http://ard.bmj.com/content/early/2017/01/20/annrheumdis-2016-210597 Back to the SIJ next time - it's taking ages to read, digest and formulate an opinion on the information but I am finding it really interesting.
0 Comments
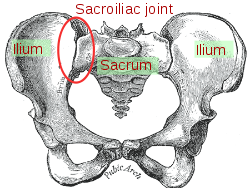 The sacroiliac joint is a mysterious beast. Many people don't know they have one...let alone 2. As the name suggests they sit between your sacrum and ilia, To put that in perspective the sacrum is the triangular bone made of (usually) 5 fused vertebrae, which in turn provides a base for the flexible bit of your spine and sits above your coccyx. The ilium (singular for ilia) is the top bit of your ironically named innominate bone (ironic as innominate means un-named and that is its name).
The sacroliliac joint does not move much, in fact, for years much of the medical profession said that it didn't move at all in adults over 40, most osteopaths disagreed vehemently. So what is the truth and why does it matter? The truth is that the joint, in most people, is very robust, the ligaments holding it together are often cited as the strongest in the body and the joint has large articular surfaces which are rough and are keyed together greatly reducing the chances of movement of one against the other. In cadavers there is a tendency for tissues to be less stretchy and as such the sacroiliac joints do appear immobile, hence the previous medical consensus that they fuse in old age. Many osteopaths, myself included are convinced we can feel a pelvic torsion, where one sacroiliac joint has rotated anteriorly or posteriorly, or slipped in the vertical plane versus the other, twisting the pelvis. We use bony landmarks and judge whether they are at the same height as the other side front and back to make our assessment. Often the discrepancy can feel quite extreme and can appear to result in a leg length difference and can result in the base of the spine appearing twisted or at an angle to the vertical, which in turn can cause a scoliosis. Scientists have been trying to work out what is happening and whether what we feel is what we think we feel. Over the next couple of weeks I will be reviewing the research I can find on the matter and presenting to you what I find...It may be I have alter my explanations of what I am finding and what I am doing to change that.  If you see me walking to and from Vauxhall, Oval or Nine Elms you'll notice that I am carrying a large and well stuffed rucksack. As well as a laptop, a couple of gowns for those patients who require one and an emergency kagoul it contains a green man-bag filled with very important things. I rarely need to use most of them and they weigh altogether almost as much as my laptop and take up an annoying amount of space. What is in this man-bag that is so important that I lug it around despite almost never needing it? The manbag contains my clinical medical kit. Inside there is:
I always ask new patients about their general health at their first visit. Asking questions about urinary continence may seem invasive and irrelevant to someone who has come in with back pain but it may be that the patient has dangerously compressed nerves in their spinal canal and further sensory and motor testing may add weight to this hypothesis. Headaches may be related to a neck dysfunction or could be something more sinister which may be implicated with a cranial nerve test. I was very grateful to have the kit this week. A patient who I have been treaing for some time and who has neck pain which is almost certainly due to mechanical injury and resultant inflammatory process but who also suffers dizziness and is therefore treated as though it might not be, had been to see another medical professional who had taken the blood pressure in both arms and found the diastolic pressure wildly 40mmHg different, they had declined to treat her and were writing to the GP. There are a number of potential reasons for wildly varying pressures but amongst them is aortic disection. This can be catastrophic and can present with jaw, neck and shoulder pain as the patient was reporting. Without the kit I would have had to refuse treatment also. I checked the pressure twice with the anaroid sphygmanomometer and once to confirm with the electronic device. The diastolics were similar and normal and, whilst the systolic was slightly higher one side on the electronic reading it was a normal difference. I did an abdominal exam to check for a spreading abdominal pulse and found nothing abnormal. Coupled with the fact that the jaw pain was a recurring condition over several months I felt confident to continue gentle treatment. So why was the other reading so different? I wwasn't there but the likelihood is that the other reading was taken in a position where perhaps the venous return from the arm was being temporarily compromised by a tight muscle, perhaps pec minor. My testing has allowed me a degree of confidence in my patient's underlying health that has allowed me to treat them and in this case to greatly reduce their pain, nevertheless it is possible that their is something seriously wrong that is only exhibiting intermittently and for that reason I will check both arms for the next few visits and support the other professional's assessment that she should see her GP. 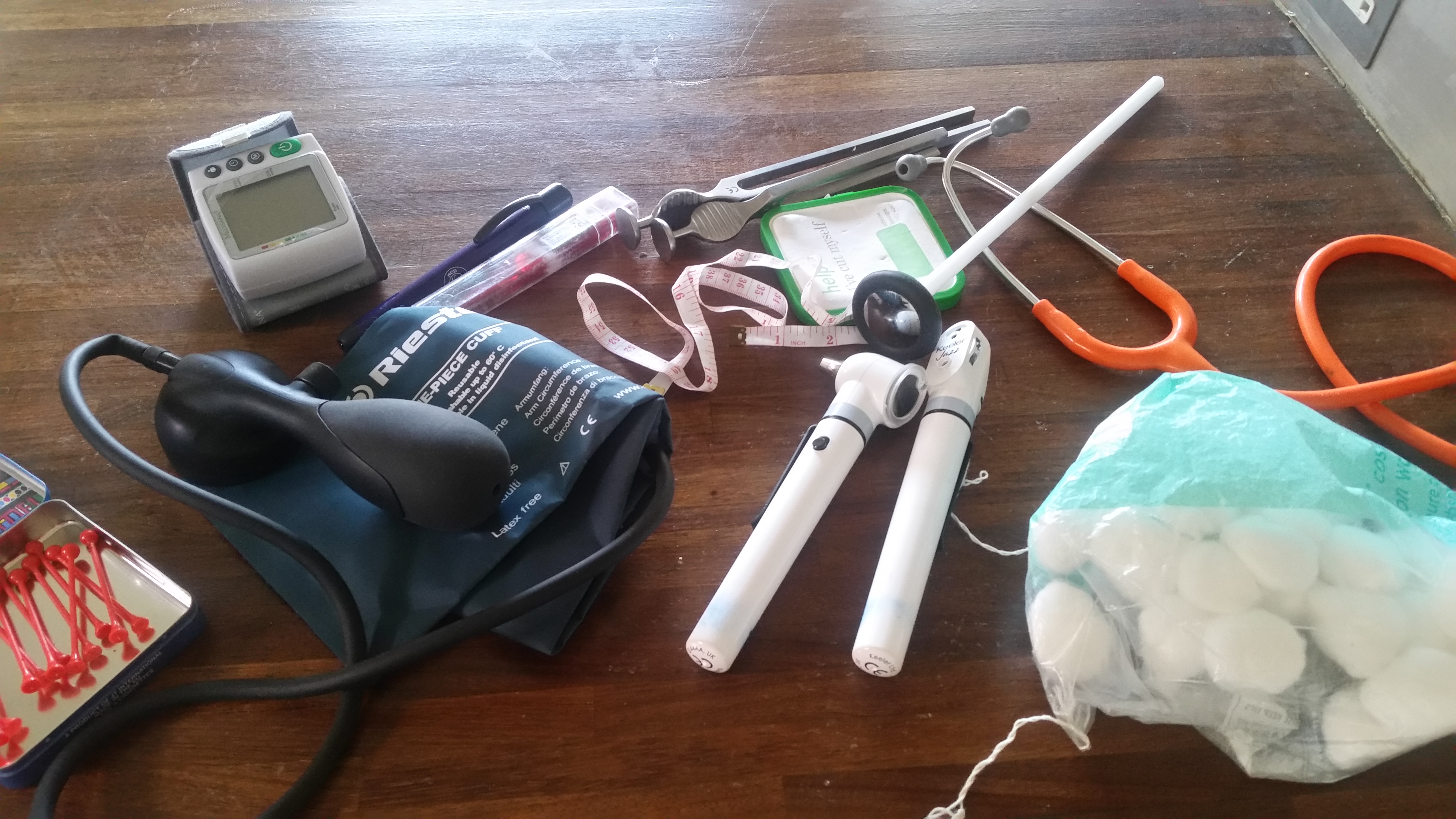 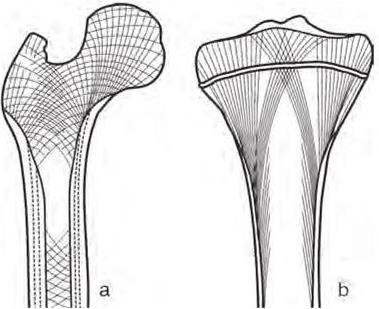 There were some lovely lightbulb moments when studying to become an osteopath, none more so than when we talked about A.T. Still's (the founder of osteopathy) assertion that structure governs function and vice versa. This is one of the basic tenets of osteopathy and is such a simple idea and yet so elegant and indeed really powerful. Modern architects, and industrial designers talk about form following function...but in the body it is so much more. You may think a baby is like a mini adult, if you were to see a baby's skeleton it would just be that of a small person. Not so. Much of the intricate structure of the skeleton is laid down as done in response to the forces that pass through it. The size of muscle attachments depend on the forces they are required to cope with, as do the overall shape density and internal geometry of long bones. Our activities carry on changing our body's structure all the way through out life. Too much time staring at a badly positioned screen and you can end up with a head forward posture, work out a lot and you'll get bigger muscles and muscle attachments.
The structure of the your body and the elements within it also dictate the limits of its function. You can't bend your elbow far in the extended direction because the olecranon hits the base of the olecranon fossa. If it didn't then you'd almost certainly damage soft tissues, blood vessels and nerves, so it's a good job all in all! As we get older we can become more and more limited as our structure becomes further and further from the ideal. A really good example of this is the head forward rounded shoulder posture of the typical office worker. The head is heavy, so once it sits anteriorly gravity tries to pull it further so. As it comes forward and the upper back starts to round, so the shoulders start to move so they sit more forward. Shoulders are not designed to sit protracted like this. Like every other joint they have compromised range of movement for stability, protection and to provide muscle attachments. If your shoulders are sat where they should be there is no bony encumbrance to raising your arms out to the side and nearly to pointing vertically (actually this is a slight simplification because your arm does a little trick to avoid one but to all intents and purposes...). If the shoulder is tipped forward then so are all the structures. You want to reach straight up but to the shoulder that is reaching up and back...try it now, you can only get to about 80'. Rounded shoulders also internally rotate the arms meaning if you want us the hands in the neutral position you have to externally rotate the forearms which can lead to tight muscles and repetitive strain injury and can also alter cause both blood and nerve supply to become restricted leading to pain, numbness, tingling and even loss of function. As usch the change in structure can have a very profound effect on function both directly and perhaps indirectly. If the back is curved like that for long enough the vertebrae will start to wedge and it will not be easily reversed and in some elderly patients osteoporotic crush fractures have caused the vertebrae to wedge significantly. For many of us though it is still early enough days to correct our rounded shoulders and our head forward some relatively easy exercise and stretches, a well adjusted workstation and some mindfulness about posture can all help significantly...oh and some help from your osteopath might not go a miss. As osteopaths we believe that it is important that joints are meant to move and that they require movement to remain healthy. Much of the treatment I give is about getting joints moving that aren't, and rebalancing the tone of tissues such as muscles around the joint so that impediments to full and free movement of the joint are reduced. The 'cure' comes from the movement and the body's response to that movement, recalibrating its neutral position, pumping away waste and replenishing nutrients. Rome wasn't built in a day but today is as good a day as any to start thinking about the small changes to the structure of your body which limit function and asking yourself how you might reverse them  Those in the medical professions have long known that actually paracetamol is not an anti-inflammatory and therefore of less use than non-steroidal anti-inflammatory drugs (NSAIDs) but it has continued to be propounded for pain by, amongst others, NICE, especially for those patients with stomach problems or other reasons to avoid NSAIDS. Cochrane are a great organisation who specialise in systematic reviews, looking at all of the available evidence, sifting, grading and weighting it and producing a definitive synthesis with a grading for how strong the evidence is. Recently they conducted a systematic review on how effective paracetamol is for acute low back pain...it isn't...at all and the evidence is strong, read the review here. A blog Cochrane have published by a major contributor goes further (here)...it appears that there is evidence for very little pain relief from paracetamol. There is some good news though (here), as I posted in an earlier blog, Cochrane studied topical NSAID gels of Diclofenac, Ibuprofen and Ketaprofen, and some Diclofenac patches provide effective pain relief...and of course won't irritate the stomach. So! If you have a bad back you might want to reach for the gel rather than a pill and if that doesn't work, of course, call for your osteopath.
 Osteopathy is not a risky business, whatever some professional sceptics may have you believe. A comprehensive study of available literature, conducted in 2009 found that serious adverse events did occur that were associated with osteopathic treatment but they were very rare. The most serious of these were strokes associated with damage to the arteries of the neck following an upper neck manipulation.
Risks of major adverse events, such as stroke with neck manipulation, are very low. Estimates suggest around 1 per 100,000 to 1,000,000 manipulations or 1 per 50,000 to 100,000 patients. To put this in perspective, the risk of having a stroke without a manipulation is around 100 strokes per 100,000 (or 1 per 1,000 people) in the general population in the UK over a one year period. you can read the study here if you wish. But that doesn't tell the full story. Those are serious adverse events associated with neck manipulations but that could be like saying going to the shops makes you fat because you notice that the more often you go to the shops the fatter you get. Of course it is not shopping that makes you fat, it is eating the chocolate bars you buy at the shop that makes you fat but there is a correlation because if you go out to buy chocolate bars more often and then eat them you both visit the shop more often and get fatter. So appears to be the case with neck manipulations and artery damage leading to stroke. A new review of the literature, read it here finds evidence that the linking variable is likely to be neck pain or headache and that some patients with a dissecting artery present at the therapist with neck pain or headache and are treated but that the neck pain/headache is the true symptom of the dissecting artery and the manipulation has no effect on it. There is a lovely table at the end of the paper showing Hills criteria for causality which clearly shows on how many counts cervical manipulations fail to qualify as causal for dissecting arteries. This is good news but is unlikely to change how I practice in the short term. I will still take a detailed case history so I am aware of the likelihood of any conditions pertinent to my treatment of you and I will still exercise caution in the treatment of anyone at risk of cardiovascular disease or connective tissue disorders or indeed with any anticipated bone weakness.  ,Hip snapping syndrome - the name conjures up images of kids from the 1960s clicking their fingers in time to cool beats. Sadly it's not so much fun. Hip snap is that funny click some people get when they straighten their legs from the hip. If you have it is likely to be irritating or perturbing, it can even be painful. It is caused by one of three things: Most commonly it is the tendon of one or more of the muscles which you use to lift your leg out to the side (and to keep your pelvis level whilst walking) flicking over your greater trochanter, that is the bony bit you can feel on the outside of your 'hip'; less commonly it is the shared tendon of two of the muscles you use to bend forward from the hip (or do the last part of sitting up) flicking over another bony prominence called the lesser trochanter; finally it can sometimes be due to internal damage within the hip joint itself.
In the case of internal damage it is likely to be a case of rest and allow the damage to repair or potentially even surgical intervention if that doesn't happen and the condition is painful, but the vast majority of patients have the extra-articular type simply caused by a tendon flicking over a bony prominence. In most cases a snapping hip is not painful but wherever one tissue rubs against another there is the potential for irritation and inflammation and in this case it is the fat pads designed to protect the tendons from the bony bits that get inflamed; bursitis can be very painful. So why does this happen? There may be (usually very minor) underlying bio-mechanical issues, one leg longer than the other or a slight torsion in the pelvis, or the tendons may be under increased tension because the muscles to which they belong are shortened or held in tension, either because of over-training, unaccustomed exercise or, ironically lack of muscle tone. All of these are potentially quite easy fixes...even the leg length discrepancy may be resolved with an over the counter heel-lift for the shoe. Why would you bother to get this sorted? You may well decide not to, if it is minor and not painful...but...If it is indicative of a leg length discrepancy or a pelvic torsion then sooner or later that is likely to affect your back and if it is due to over training your muscles surely you'd want to know and redress the balance before you cause other problems, likewise if particular muscles are not firing properly, that will affect the energy required to walk and may lead to future back and knee issues, finally, of course, it would be better not to let it develop into bursitis as that can take some time to resolve. Snapping hip isn't serious but it is a great early warning sign to get things checked out to stop it becoming something else.  Unlike type I osteoporosis which affects post-menopausal women, type II affects men and women in old age. Scientists noticed that there was a causal effect between mice having low levels of mesenchymal cells and developing type 1 osteoporosis, so they wondered whether the introduction of mesenchymal cells from healthy mice would reduce bone or halt deterioration. Amazingly the bone regenerated, with the damaged delicate interior structure (trabeculae) of the bone re-forming into healthy functioning bone. Further studies are required but this really is exciting news and may pave the way for treatments whichdelay the onset of old-age osteoporosis, possibly indefinitely. If you want a bit more detail the abstract is here
 I am no fan of soy milk. Let me be honest, when I go to someone's house and they offer me tea with soy milk I die a little on the inside. I know some people can't digest, or find it hard to digest dairy products and some are vegan out of principle but there is a reactionary bit of me that screams 'it's a fad' every time I see soy milk. Well aren't I the fool? it turns out those soy chai latte swilling hipsters were onto something (to be fair it is a staple in many Asian diets not just for the bearded ones). Recent research published in Rheumatology International showed a very significantly lower incidence of osteophyte (bony outgrowths that are one of the main indicators of osteoarthritis) development in members of the study group (5764 Chinese patients over 40 attending for a weight-bearing knee x-ray as part of a routine checkup). Interestingly joint space narrowing (indicative of loss of articular cartilage was not affected). It is too early to say what the implications are but I may occasionally swallow my prejudices and take the soy option from here on in.
 You may not be as fat as you think you are. No, seriously, and I'm not talking about body dysmorphia, although that is another important topic. No, this time I am talking about how the anterior posterior curves of your spine and the tilt of you pelvis can affect how prominent your abdomen is. This is a subject dear to my heart...well, my tummy. Just as the spine can develop lateral curves (scoliosis), so the anterior posterior curves can vary also and just as a scoliosis can be due to bony architecture and permanent (to a greater or lesser degree) or can be due to temporary or recent soft tissue changes and can be more amenable to change so can anterior posterior curves.  There are several different categorisations of different back shapes, this is the one I was taught...I admit I objected to the terminology 'ideal'...because mine isn't preferring the term 'ordinary' with the slight implied dullness, but the truth is 'ideal' is ideal for weightbearing and good function of the body. If you look at kypho-lordotic you will see that even in these diagrams it is drawn with a protruding tummy. It is actually very hard to arch the small of your back without sticking your tummy out. If you ask a child to stick their tummy out they will do just that. Not only does the kypjo-lordotic posture push out the tummy it rounds the back which naturally encourages the shoulders to round in from the sides (so you have round shoulders) and makes you crane your neck which can cause problems there, so all in all, not ideal, however dull that may be. So can anything be done about this? The short answer is yes. How much change can be effected depends on what is causing the posture, how much time, effort and resource you are willing to commit and how adaptable your body is. Sometimes the problem is very acute and has occurred because of a recent injury perhaps a minor facet joint or rib lesion injury that is bending over your upper back (kyphosis) and causing you to arch the lower back to bring our head up level, sometimes the hip flexors (especially psoas), or muscles in the low back are too tight, maybe due to over training or poor training, and are pulling the low back into extension, or indeed there could be a minor joint injury in the low back or even the pelvis. These problems are usually easily resolved with treatment. Sometimes the problem is due to poor habits and soft tissues in general have shortened in these positions, these the patients may have to commit to a longer period of treatment and/or changed behaviours and stretching/exercise routines. For some, there may be bony changes, wedging of vertebrae. This is common in the elderly, but also (usually in a minor way) in teenagers who especially those who grow very quickly. For these patients we would expect a smaller margin of improvement, the possibilities are limited but gravity will be constantly trying to increase the curve so there is likely to be room for improvement. More importantly internal organs from the lungs to the digestive system (reflux etc) to the bladder are strongly affected in their roles by changes in posture and the pressures that exerts...a small change may make a big difference to quality of life. I mentioned this being important to me. I think I always had a tendency to push out my belly and I've had a niggling injury that causes my upper back to be more rounded than I'd like. So I have been receiving osteopathic treatment and exercising to try and reduce my kypho-lordotic posture. I know it is working because I haven't lost weight but now some of my trousers that were tight are loose and shirts that didn't fasten now do comfortably. For me some of my belly was definitely from my back...for Mr Greedy I am not so sure
|
Archives
February 2024
AuthorDamian is the principal osteopath at Vauxhall Village Osteopathy and Oval Osteopathy Categories
All

|

|

|

|
 RSS Feed
RSS Feed